INVERSION ANKLE SPRAIN
Carley Maanika, ATS
Kelley Galloway, ATS
Jessica Krali, ATS
Northern Michigan University
Pathology, Diagnosis, and Getting On Track with Rehabilitation
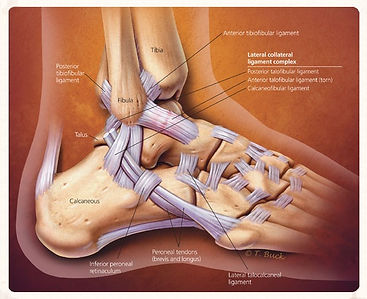
ANKLE ANATOMY
The anatomy of the ankle includes bony, muscular, and ligamentous aspects. The ankle is actually made up of three joints; the subtalar joint, the talocrural, or and the inferior tibiofibular joint (Prentice 2011).
The bony anatomy of the ankle includes three bones: the tibia, fibula, and talus. There are twenty muscles in the foot that control movements. The main muscles that affect the ankle are the anterior tibialis, posterior tibialis, the peroneals (longus, brevis, tertius, extensor digitorum longus and brevis, flexor digitorum longus and brevis, flexor hallicus longus and brevis, and extensor hallicus. Additional injuries to these structures, primarly the peroneus longus and peroneus brevis, can occur in conjuction with a lateral ankle sprain.
Inversion (supination) and eversion (pronation) occur at the subtalar joint in the ankle. This joint is made up of the articulating surfaces of the talus and the calcaneus, the two biggest tarsal bones in the foot (Prentice 2011). The anterior talofibular ligament’s purpose is to prevent anterior subluxation of the talus during motion. Similarly, the posterior talofibular ligament prevents posterior subluxation of the talus. The third lateral ligament, the calcaneofibular ligament, prevents excessive inversion.